
Hydrocephalus and Seizures — Understanding Why They Happen and How Families Manage Both

The first seizure happened three weeks after my son’s shunt surgery. I was in the room. He was lying on the bed and suddenly something changed — a stiffness, a tremor, his eyes rolling. It lasted less than a minute. It felt like an hour.
We were back in hospital that same night. By the next morning, there was a second diagnosis to learn: epilepsy, secondary to the hydrocephalus. Two conditions. Two medications to understand. Two separate sets of warning signs to memorise.
If this is where you are — managing both — this article is for you.

The Connection Between Hydrocephalus and Seizures
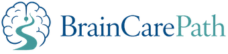
Hydrocephalus and epilepsy are not the same condition, but they are frequently connected. Understanding why helps.
The brain’s neurons — its electrical cells — function within a delicate chemical and pressure environment. When that environment is disrupted — by excess cerebrospinal fluid, by the damage that pressure can cause to brain tissue, by surgery, or by the underlying condition that caused the hydrocephalus in the first place — the electrical firing patterns of neurons can become abnormal. This abnormal firing is what a seizure is.
In children with hydrocephalus, seizures can arise from several sources: the elevated intracranial pressure itself, structural changes to brain tissue caused by prolonged pressure, surgical intervention (the brain is an organ that does not experience surgery without some adjustment), orThe original cause of the hydrocephalus — such as an infection, a bleed, or a congenital structural difference.
Studies suggest that between 15% and 30% of children with hydrocephalus will experience seizures at some point. In children whose hydrocephalus was caused by meningitis, intraventricular haemorrhage, or significant brain malformations, the rates are higher.
This is not a small percentage. It is not unusual. It is something neurosurgical and neurology teams are experienced in managing together.
What a Dual Diagnosis Means in Practice
When a child receives both diagnoses — hydrocephalus and epilepsy — the family enters a new kind of management complexity. The conditions interact in ways that are important to understand.
Shunt function affects seizure risk. When a shunt begins to fail and pressure rises, seizures can increase in frequency or intensity. A change in your child’s seizure pattern — more frequent, longer, more severe — should always trigger an assessment of shunt function, not only epilepsy management.
Seizures can look like shunt malfunction, and vice versa. Both can cause drowsiness, vomiting, and reduced responsiveness. Distinguishing between them matters because the responses are different. Your neurology and neurosurgical teams need to communicate with each other — make sure they do.
Levetiracetam — What It Is and What Families Actually Experience
My son was prescribed Lerace Syrup — the liquid formulation of levetiracetam — after his first seizures. We learned to measure it precisely. Levetiracetam (Keppra, Lerace) is one of the most commonly prescribed first-line AEDs in paediatric neurology.Behavioural changes are the most commonly reported concern.Sleep disruption and Fatigue are also reported.

What This Means for Your Family
Navigating a dual diagnosis is hard. Finding a neurologist and neurosurgeon who speak to each other is key.
This article is written for informational purposes only and does not constitute medical advice. Always consult your neurologist, pediatrician, or qualified healthcare provider for diagnosis and treatment decisions specific to your situation.