We had twenty minutes with the neurosurgeon.
Twenty minutes to understand what was happening inside my son’s brain, what the surgery would involve, what the risks were, what recovery looked like, and what the rest of his life might hold.
I had not slept properly in four weeks. I was running on fear and adrenaline and the desperate hope that this doctor had answers. I sat across from her and I could not think of a single question to ask.
I nodded. I signed the forms. I walked back to my son’s room and sat beside him and realised I understood almost nothing.
This article exists because of that moment. Every question on this list is one I wish I had asked. Some I found the answers to later — in research papers, in parent forums, in conversations with other families. Some I am still learning the answers to today.
Before your next neurosurgery appointment, print this list. Take it with you. You do not have to ask every question in one visit. But knowing which questions matter will help you use the time you have.

Before Surgery
1. What type of hydrocephalus does my child have, and does the type affect which treatment you recommend?
There are several types of hydrocephalus — communicating, non-communicating, normal pressure, and others. The type matters because it influences whether a VP shunt, an ETV, or another approach is most appropriate. Not every surgeon will explain this distinction unless you ask.
2. What are the specific risks of surgery for my child — not risks in general, but risks given their age, condition, and current state?
General risk statistics are useful context. What matters more is how those risks apply to your specific child. A surgeon who has reviewed your child’s imaging and case history should be able to speak to this specifically.
3. Are you recommending a VP shunt or an endoscopic third ventriculostomy — and why?
Both are established treatments. ETV is less invasive and avoids the long-term complications of shunt hardware — but it is not appropriate for all types of hydrocephalus. If your surgeon is recommending a shunt without discussing ETV, it is reasonable to ask why ETV is not being considered.
4. How many of these procedures have you performed, and what are your outcomes?
This is not an impolite question. It is one of the most important questions a parent can ask. Surgical outcomes are directly related to surgical experience. A neurosurgeon performing paediatric hydrocephalus surgery regularly will have better outcomes than one who does it occasionally.
5. What will you be looking for in the imaging before deciding on the exact surgical plan?
Understanding what the surgeon sees in the MRI or CT scan — and what information guides their decisions — helps you understand the process and ask better follow-up questions.

About the Shunt (If Recommended)
6. What type of shunt are you recommending and what are the differences between shunt types?
There are fixed-pressure shunts and programmable shunts. Programmable shunts can be adjusted non-invasively after surgery — which can prevent problems related to overdrainage. Ask which type is planned and why.
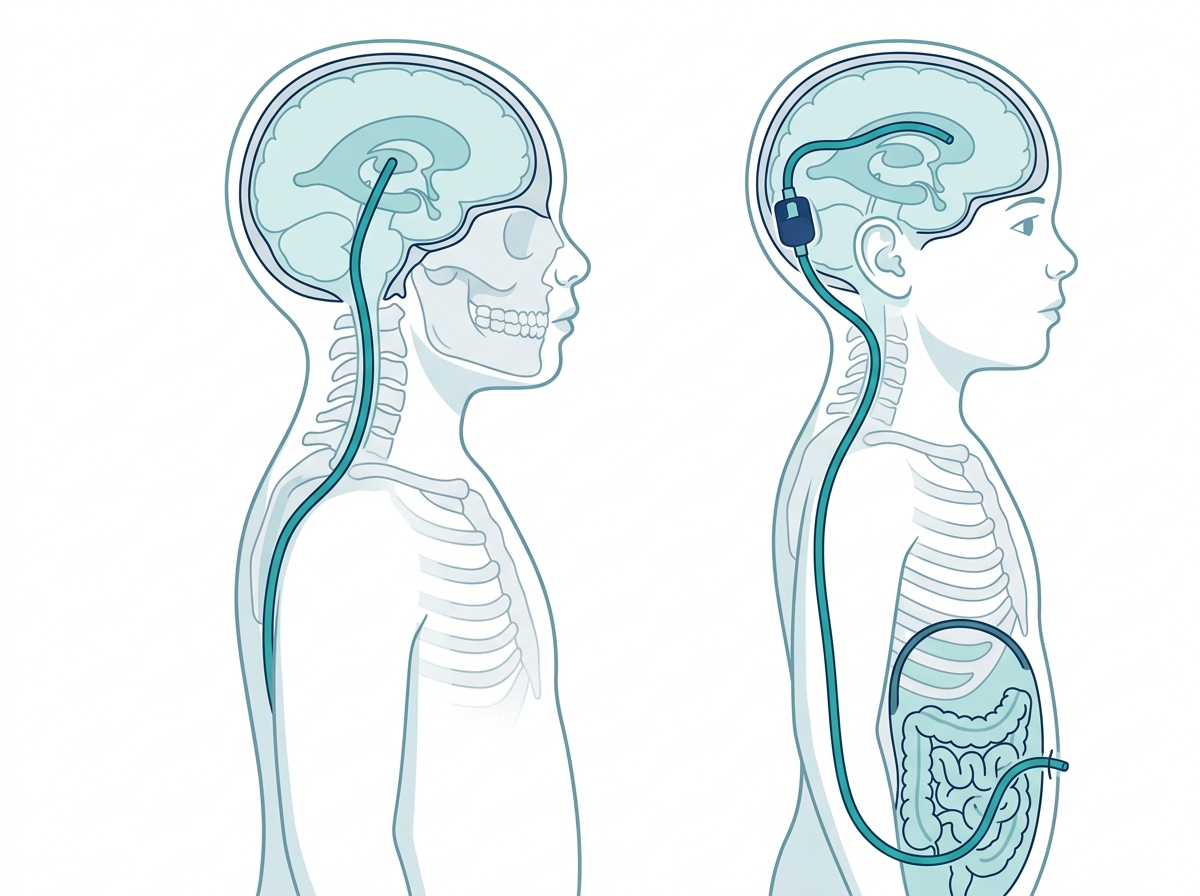
7. Where will the shunt drain to — the abdomen, the heart, or somewhere else?
Most VP shunts drain to the peritoneal cavity (abdomen). In some cases, other sites are used. Understanding this helps you know what to watch for and where.
8. How will I know if the shunt is failing?
Shunt failure is the most common complication of hydrocephalus surgery — occurring in up to 40% of cases within two years. The symptoms of shunt failure are specific and it is essential that every parent can recognise them. Ask your surgeon to describe them clearly and ask what to do — and where to go — if you suspect failure outside of clinic hours.
9. What is the average lifespan of the shunt you are placing, and what happens when it needs replacing?
Shunts are not permanent devices. They may need revision surgeries over a child’s lifetime. Understanding this early helps families plan and reduces shock when revision becomes necessary.
About Recovery
10. What does the recovery timeline look like — not the best case, but the realistic case?
Ask for honesty here. Surgeons sometimes present optimistic timelines. What you need is a realistic expectation — including the possibility that recovery may be slower or more difficult than hoped.
11. What symptoms after surgery are normal and which ones mean I should bring my child back immediately?
There is a difference between expected post-surgical discomfort and warning signs of complications. Know specifically which symptoms require urgent attention and who to call.
12. When can my child return to normal activities — and are there activities they should avoid long-term?
Contact sports, swimming, air travel — parents have practical questions that affect daily life. Ask about specific activities relevant to your child’s age and lifestyle.
About the Future
13. What developmental outcomes should I realistically expect, and what factors influence those outcomes most?
This is perhaps the hardest question to ask — because the answer may be uncertain or difficult. But a frank conversation about developmental expectations helps families access the right early intervention services and set realistic goals.
14. How often will my child need follow-up appointments, and what will those appointments involve?
Understanding the monitoring plan — imaging frequency, clinic visits, what is being watched for — gives parents a framework for the years ahead.
15. What support resources do you recommend for our family — including for us as parents, not just for our child?
A good neurosurgeon will know that hydrocephalus affects the whole family. They should be able to direct you toward parent support groups, social workers, psychological support, and community resources. If they cannot, ask your GP or paediatrician instead.

Practical Tips for the Appointment
Bring someone with you. A second person — a partner, a parent, a trusted friend — will hear things you miss and remember things you forget.
Write questions down before you go. The ones that feel obvious at home become impossible to remember in the consulting room.
Record the appointment if the surgeon permits. Many will agree to this. It means you can review exactly what was said, in their exact words, after the stress of the moment has passed.
Do not apologise for asking. Every question on this list is reasonable and professional. A neurosurgeon who makes a parent feel foolish for asking about their child’s treatment is not demonstrating good care.
Ask for written information. If the surgeon mentions a specific shunt type, a specific risk percentage, or a specific timeline — ask if there is written material about it that you can take home.
After the Appointment
Write down everything you remember as soon as you leave. Include anything that surprised you, anything that was unclear, and anything you wish you had followed up on. These notes become the foundation of your next appointment’s questions.
The medical team knows hydrocephalus. You know your child. The best outcomes happen when both kinds of knowledge are in the room together.
This article is for informational purposes only and does not constitute medical advice. Always consult your child’s neurosurgeon and medical team directly. Read our full medical disclaimer at braincarepath.com/disclaimer/
Bibliography
- Drake JM, Kestle JR, Milner R, et al. Randomized trial of cerebrospinal fluid shunt valve design in pediatric hydrocephalus. Neurology. 1998;51(4).
- Kestle JR, Drake JM, Cochrane DD, et al. Lack of benefit of endoscopic ventriculoperitoneal shunt insertion: a multicenter randomized trial. Journal of Neurosurgery. 2003;98(2):284-290.
- Kahle KT, Kulkarni AV, Limbrick DD Jr, Warf BC. Hydrocephalus in children. Lancet. 2016;387(10020):788-799.